
- Coronary anatomy
- What is coronary artery disease?
- Symptoms of Coronary Disease
- How is it diagnosed?
- How is it treated?
- Helpful Links
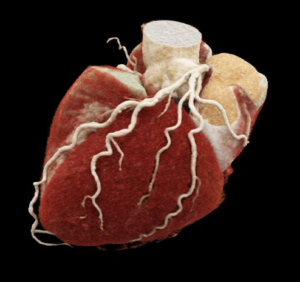
Coronary anatomy
Coronary arteries supply blood to the heart muscle itself. They are the first branches attached to the main artery which leaves the heart- the aorta- and sit like a crown on the heart’s surface hence the name coronary. There are two main arteries the left and the right each of which have numerous branches. The left coronary artery has two main branches – the left anterior descending (LAD) which goes down the front of the heart and the left circumflex (LCX) which travels around the back (posterior) of the heart. The right coronary artery travels on the right hand side and goes to the underside of the heart (inferior). Healthy arteries have considerable reserve capacity and symptoms of inadequate blood supply usually only occur when the diameter of an artery is reduced by 70% or more.
The artery has 3 layers in the wall: an inner lining layer – the endothelium -which when healthy acts as a non-stick surface, a middle layer, which contains a lot of muscle (the media), and an outer, reinforcing layer – the adventitia.

Normal coronary arteries
There are variations in normal coronary anatomy which are often harmless but in some cases the unusual course they take can cause problems such as when the coronary artery passes between the two arteries which leave the heart – the aorta and pulmonary artery.
What is coronary artery disease?
The arteries have a large amount of muscle in their wall which can go into spasm, restricting blood flow, but usually it is the slow build-up of cholesterol and scar tissue underneath the lining layer of the artery, or ‘endothelium’, which eventually leads to inadequate blood flow – stable coronary disease. Alternatively this may occur suddenly when a cholesterol rich plaque develops a crack in the surface layer leading to blood clot formation and the acute coronary syndromes (ACS) of unstable angina, acute myocardial infarction (‘heart attack’) and sudden death.

Progression of coronary artery disease
Coronary artery disease starts to develop in the teens and early 20’s before showing up with symptoms in the 40’s to 60’s.
The key to prevention is to change lifestyle early in life but no matter how old you are a change in lifestyle is beneficial.
Symptoms of Coronary Disease
When the condition develops slowly there is time to find it and treat it.
The classical symptom is discomfort in the chest, throat, jaw, teeth or arms which occurs on exertion or emotional stress. These symptoms which are short lived – lasting only two to 5 minutes – are often described as ‘heavy’, ‘pressing, constricting’ or ‘burning’. They may resemble ‘indigestion’. Classically, angina is more likely to occur with exertion earlier in the day, after meals or in extremes of temperature or humidity. Typically it is not painful but does have a sinister or worrying quality.
Some patients experience symptoms which are angina ‘equivalent’ which means breathlessness on exertion which is more obvious suddenly or varies with the time of day or eating for example.
Symptoms of angina can underestimate the extent of coronary artery disease. About 80% of episodes of inadequate blood flow to the heart are completely silent or ‘asymptomatic’, but can be detected by ECG recordings during daily life.
How is it diagnosed?
How is it diagnosed?
Symptoms and clinical context remain central to diagnosing coronary artery disease. A key first step is separating stable from unstable presentations. Stable coronary disease usually develops gradually and tends to carry lower immediate risk, whereas unstable coronary disease can represent an evolving heart attack and is a medical emergency requiring prompt assessment and treatment.
Although a heart attack (acute myocardial infarction) is often painful, it can present atypically or with minimal pain, particularly in people with diabetes, in older patients, and around surgery or shortly afterwards. As with many medical conditions, the diagnosis is made by bringing the story and examination findings together with test results, rather than relying on any single test.
Electrocardiogram (ECG)
A standard ECG can show evidence of prior heart damage or suggest reduced blood supply to the heart muscle. It is often most informative when compared with previous ECGs. Importantly, an ECG can be normal even when coronary disease is present, so results are interpreted in the context of symptoms and other findings.
Blood tests (cardiac biomarkers)
Blood tests for heart muscle injury, most commonly troponin, are essential when a heart attack is suspected. Troponin can also be elevated in other conditions, so the result needs to be interpreted alongside symptoms, ECG changes, and the pattern of rise and fall over time.
Stress testing (functional assessment)
Stress testing assesses whether symptoms are due to reduced blood flow to the heart muscle. It may involve exercise on a treadmill or bicycle, often combined with imaging such as stress echocardiography or nuclear perfusion imaging (“cardiac sestamibi scan”). For patients who are unable to exercise adequately, pharmacological stress tests may be used.
Stress tests are particularly helpful when symptoms suggest coronary disease but the likelihood of a significant blockage is uncertain, or when we need to assess whether known coronary disease is causing ischaemia.
Coronary CT and CT coronary angiography (CTCA)
Coronary CT has become an important part of modern assessment, particularly for patients with stable symptoms and an intermediate probability of coronary disease.
Calcium scoring is a quick, low-radiation CT scan that detects calcified plaque. It can be useful for refining risk in asymptomatic patients or those with atypical symptoms. A calcium score of zero is reassuring in many people, but it does not exclude non-calcified plaque.

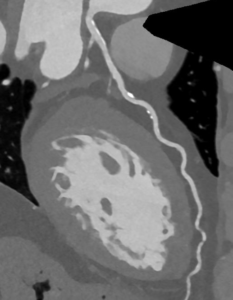
Calcium Score Scan (without contrast) showing calcified plaque in the main coronary vessel (LAD). The degree of narrowing (stenosis) cannot be ascertained from this scan without contrast injection, however a risk calculation can be made based on the total amount of calcium adjusted for age and sex.
CT coronary angiography (CTCA) is a contrast CT scan that directly images the coronary arteries. It can detect both calcified and non-calcified plaque and determine whether there is narrowing of the vessel lumen. In appropriate patients, CTCA is an excellent test to assess coronary anatomy and can often avoid more invasive testing.
CTCA provides a detailed snapshot of the coronary arteries at a point in time. It is not routinely used for serial monitoring in most people, and treatment decisions are usually guided by symptoms, overall cardiovascular risk, and response to therapy.
In selected patients, advanced analysis of CTCA can provide deeper information about plaque burden and biological risk signals (see CaRi-Heart link). This can help refine preventive strategies beyond what is possible from stenosis assessment alone.
A Photon-Counting CT coronary angiogram reconstruction of the left anterior descending (LAD) artery from the same patient. The lumen and degree of stenosis (narrowing) can be accurately assessed with the aid of contrast dye at high resolution, demonstrating both calcified and non-calcified plaque.
Cardiac MRI
Cardiac MRI is often used when the key clinical question relates to the heart muscle, such as assessing heart function, prior infarction (scar), myocarditis, or in some cases inducible ischaemia with stress perfusion imaging. It does not image the coronary arteries as directly as CTCA, but it can be a powerful complementary test, especially when assessing viable myocardium (i.e. muscle that is still alive and may benefit from restoration of flow from blocked arterial supply).
How is it treated?
As always prevention is the key with lifestyle changes such as eating less, exercising more, losing weight – particularly reshaping with loss of abdominal fat – and stopping smoking all being valuable. These can be very powerful interventions. Stopping smoking after a heart attack halves the risk of another heart attack in the next year.
Risk factors such as high blood pressure, diabetes and high cholesterol and triglycerides are managed with drugs as a supplement to lifestyle changes. Even modest weight reductions of 5-7Kg can lead to major health benefits. Changing shape is as important as losing weight. Total cholesterol levels may obscure important information about the mix of cholesterol such as the low density cholesterol particles (LDL) produced in the liver which circulate in the blood and increase risk of artery disease and the high density cholesterol particles (HDL) which recycle cholesterol deposits in the circulation and actually reduce risk. The aim of treatment is to reduce cholesterol deposition by reducing LDL. Another type of fat which is important is triglycerides (TG). These can be reduced by lifestyle changes such as weight and alcohol reduction, improving fitness, tightening diabetic control and correcting conditions such as an underactive thyroid. Fish oil occurring naturally in oily fish and taken as supplements is effective at lowering triglycerides.
There are 3 treatment options to treat coronary disease: drug treatment, balloons (angioplasty) usually combined with coronary stenting, or coronary artery bypass surgery.
We use drugs to treat the underlying coronary disease (anti-platelet drugs, cholesterol and triglyceride lowering, and blood pressure medications such as ACE inhibitors or AT2 RAs), reduce symptoms of angina or dissolve the blood clots (thrombolytics) which cause acute coronary syndromes.
Angina is treated with drugs which slow the heart rate and lower blood pressure including beta-blockers and calcium channel blockers. The traditional remedy of nitroglycerine (Anginine, Nitrolingual spray, mononitrates) is helpful to treat symptoms as they occur and is often taken preventatively such as before exertion.
Remember that most episodes of angina are ‘silent’ and so prevention of angina rather than treating symptoms as they occur is important.
Angioplasty and stenting is recommended for troublesome stable symptoms and acutely to treat heart attack. In this procedure a tube or catheter is placed in an artery in the groin (femoral approach) or wrist (radial approach) under local anaesthetic, into the opening of the coronary artery in the aorta. A wire is then passed across the narrowed section of the artery and the balloon is inflated, crushing the plaque. Usually a collapsible steel mesh is left in the artery and stays embedded in the wall. Coronary angiography and angioplasty
Coronary artery bypass surgery uses a piece of spare artery or vein to go around (‘bypass’) a partial or complete obstruction or ‘blockage’ in a coronary artery. Traditionally cardiac surgeons operated with the patient’s heart stopped for a period of time and their circulation supported with a heart:lung machine. Increasingly surgery is performed with a beating heart and often without putting a clamp on the aorta (‘anaortic’) which substantially reduces the stroke risk and other brain related complications of heart surgery. Spare veins taken from the legs or arms have been used in the past but current best practice uses spare arteries from inside the chest (left and right internal mammary arteries) or from the forearm (radial). These arteries are similar in size to the coronaries they are sewn onto, and as they are built to withstand the high pressure inside, arteries are more durable than vein grafts. www.scts.com.au