
- Heart Failure
- What is heart failure?
- What causes it?
- How is it diagnosed?
- How do we treat it?
- Prevention
- Helpful Links
Heart Failure
The heart pumps blood into the lungs (pulmonary circulation) and the rest of the body (systemic circulation) simultaneously. When healthy, the heart has the capacity to not only meet the blood flow needs of critical organs like the brain, kidneys and liver but also to increase its output to meet the changing needs of the body such as during exercise, mental stress or illness.
What is heart failure?
Heart failure occurs when the heart is unable to meet the blood flow requirements of the tissues. The heart may fail to contract with normal power (measured as left ventricular ejection fraction), initially under stress and later at rest. This is called systolic heart failure. The other type of heart failure – diastolic heart failure or ‘heart failure with preserved ejection fraction’- is due to stiffness of the heart muscle which prevents the heart from filling normally after it contracts. This occurs for example in diabetes, hypertension and with increasing age.
The body adjusts to heart failure in a number of ways which partly compensate but as the disease progresses exercise capacity falls, salt and water accumulates in the lungs (pulmonary oedema) and the rest of the body causing worsening breathlessness, liver congestion, swelling of the abdomen and legs and sleep disruption central sleep apnoea Initially people only notice these changes when exerting themselves and often think is it part of “aging” or being unfit, only seeking help when their shortness of breath becomes severe.
Some patients have a combination of both systolic and diastolic heart failure. Heart failure of either type is a serious condition which impacts on length and quality of life, but fortunately there are many treatments and lifestyle changes that can improve both survival and quality of life.
What causes it?
Heart muscle damage can be caused by a various factors. The commonest causes are coronary artery disease (‘heart attack’) and cardiomyopathy or heart muscle disease . Genes play an important role in cardiomyopathy and in coronary disease, diabetes and hypertension.
Hypertension leads to heart muscle thickening or hypertrophy and therefore stiffness. It is a common cause of heart failure with preserved contraction (previously known as diastolic heart failure). Reduced contraction occurs late in the disease.
Heart valve disease leads to narrowed (stenosis) or leaking (regurgitation) valves – most commonly the aortic or mitral valves are involved. This typically occurs gradually but can change suddenly such as when infected (endocarditis). Viral infections can affect heart muscle (myocarditis). Rheumatic fever is becoming less common.
Heart muscle can also be damaged by drugs and toxins, in particular alcohol, but also cancer drugs (Anthracyclines or Herceptin)
Obstructive sleep apnoea is increasingly recognised as a cause of heart failure.
Heart rhythm disorders can cause or worsen heart failure with atrial fibrillation, atrial flutter and, less commonly, supraventricular tachycardia. Heart Rhythm Disorders
How is it diagnosed?
Heart failure is diagnosed by a combination of symptoms (breathlessness, abdominal or ankle swelling), signs of fluid overload in the chest, abdomen and legs when examined and confirmed by evidence of abnormal heart function (either reduced contraction or preserved contraction with markedly increased stiffness). This evidence is usually obtained using cardiac ultrasound (echocardiogram).
Dilated cardiomyopathy: the heart is enlarged and its function reduced
Hypertrophic cardiomyopathy: the heart is not enlarged but is stiff – the muscle is markedly increased and the cavity smaller
A major diagnostic tool is measurement of cardiac biomarkers. These substances are released into the bloodstream early in the course of the disease and offer the promise of earlier diagnosis and treatment. The most common is BNP which is now being used to diagnose and help manage heart failure and may be used to screen for heart failure potentially earlier in the course of the disease when treatments have the greatest benefit. There are many other biomarkers such as galectin 3, ST2, and cardiotrophin which are undergoing clinical trials but are not yet clinical tools.
Other tests which are frequently used to determine whether heart failure is present and its cause include: blood tests, x-rays, coronary angiograms, CT scans and nuclear scans (SestaMIBI). Some investigations like PET and MRI scans have an emerging role but are expensive and not readily available.
Related: Invasive Cardiac Diagnostics
How do we treat it?
Modern heart failure management is a team based approach which includes the patient’s family, Family Doctor, Specialist Heart Failure Nurses and Physiotherapists (heart failure exercise programs) and is community, rather than hospital, based. A key strategy is to try to detect early deterioration of heart failure (decompensation) so that treatment can be adjusted and hospitalisation avoided.
The key elements are lifestyle changes, drugs, treatment of sleep apnoea and devices.
Lifestyle changes include smoking cessation, dietary changes (salt and alcohol restriction), fish oil supplementation, weight reduction and tailored exercise programs. Foods high in salt such as olives and anchovies need to be avoided and excessive water intake reduced. This can be difficult as thirst is increased in heart failure.
Drug treatment improves quality and length of life, proven in many clinical trials. The most commonly used are:
- ACE inhibitors (perindopril, ramipril and many others) and ARBs (angiotensin receptor blockers – irbesartan, candesartan and others) affect the Renin-Angiotensin-Aldosterone system.
- Beta-blockers (bisoprolol, carvedilol, metoprolol succinate, nebivolol)
- Aldosterone antagonists (spironolactone, eplerenone)
- Diuretics or ‘water tablets’ (frusemide, hydrochlorothiazide) are used when fluid overload (‘congestion”) occurs or is likely to.
- Anticoagulant drugs (‘blood thinners’) like Warfarin and newer drugs (Dabigatran) are needed when patients have a high risk of stroke such as those with atrial fibrillation.
- Sinus node inhibitors (ivabradine) these newer drugs which slow heart rate are currently available via a special access scheme.
Diagnosis and treatment of sleep disorders (obstructive, central or mixed sleep apnoea) is regarded as increasingly important. Newer, simpler methods of diagnosis should facilitate this and more sophisticated devices can treat the more complex sleep apnoea common in heart failure patients.
Implanted devices have two basic functions: 1) to treat arrhythmias and 2) to treat heart failure.
Defibrillators (ICDs) reduce the risk of sudden death due to serious heart arrhythmias. They are used for primary prevention in those with systolic heart failure (reduced ejection fraction) and secondary prevention when a significant asymptomatic ventricular arrhythmia or cardiac arrest has occurred.
Biventricular pacing (cardiac resynchronisation) is a heart failure treatment which can improve the efficiency of the heart’s contraction by pacing both right and left ventricles simultaneously. These devices are usually ICDs as well Defibrillators .
These devices can be used to detect changes in heart rhythm (AF) and lung water (thoracic impedance) which can predict impending heart failure decompensation.
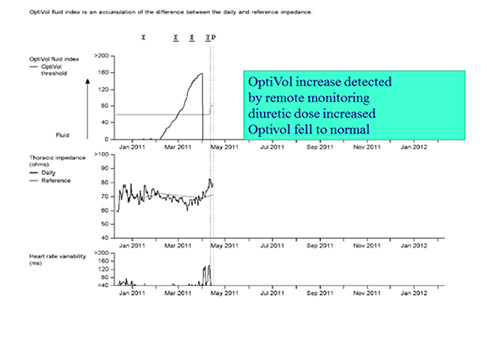
Country patient with ICD and worsening heart failure detected by remote monitoring
Prevention
Heart failure is a serious condition. Prevention and early detection are critical and have been the focus of major efforts to reduce the health burden of chronic heart failure by encouraging a healthier lifestyle and aggressively managing risk factors for heart failure (coronary artery disease, hypertension, obesity, diabetes, kidney disease, obstructive sleep apnoea).
Genetic testing will help identify those family members at risk of future heart failure due to inherited diseases like cardiomyopathy. New biomarkers should help us detect heart failure much earlier than current testing does and potentially be used in population screening.
The National Heart Foundation has lots of information on how to keep your heart healthy, prevent heart failure and how to manage heart failure if it develops.