
“AI quantitative plaque analysis (CaRi-Plaque)”
A structured, AI-enabled analysis of CT coronary angiography that quantifies plaque burden and plaque type to better define long-term risk.
Traditional coronary CT reporting has (understandably) focused on whether a plaque causes a flow-limiting narrowing. But over the last decade, it has become increasingly clear that many heart attacks arise from plaques that are not severely obstructive beforehand, and that total atheroma burden and plaque biology matter, not just the tightest stenosis.
This aligns with a broader shift in cardiology away from an exclusive fixation on “blockages” and toward non-obstructive atheroma, higher-risk plaque features, and biological activity as drivers of future events.
Related pages
• CaRi-Heart inflammation analysis (FAI) CaRi-Heart – Central Sydney Cardiology
• CSC becomes Australia’s first CaRi-Heart Centre CSC becomes Australia’s first CaRi-Heart® Centre, led by A/Prof Imre Hunyor – Central Sydney Cardiology
What is “AI quantitative plaque analysis”?
AI quantitative plaque analysis uses the CT coronary angiogram dataset to build a 3D model of the coronary arteries and then measures plaque in a way that is far more objective and reproducible than visual estimation alone.
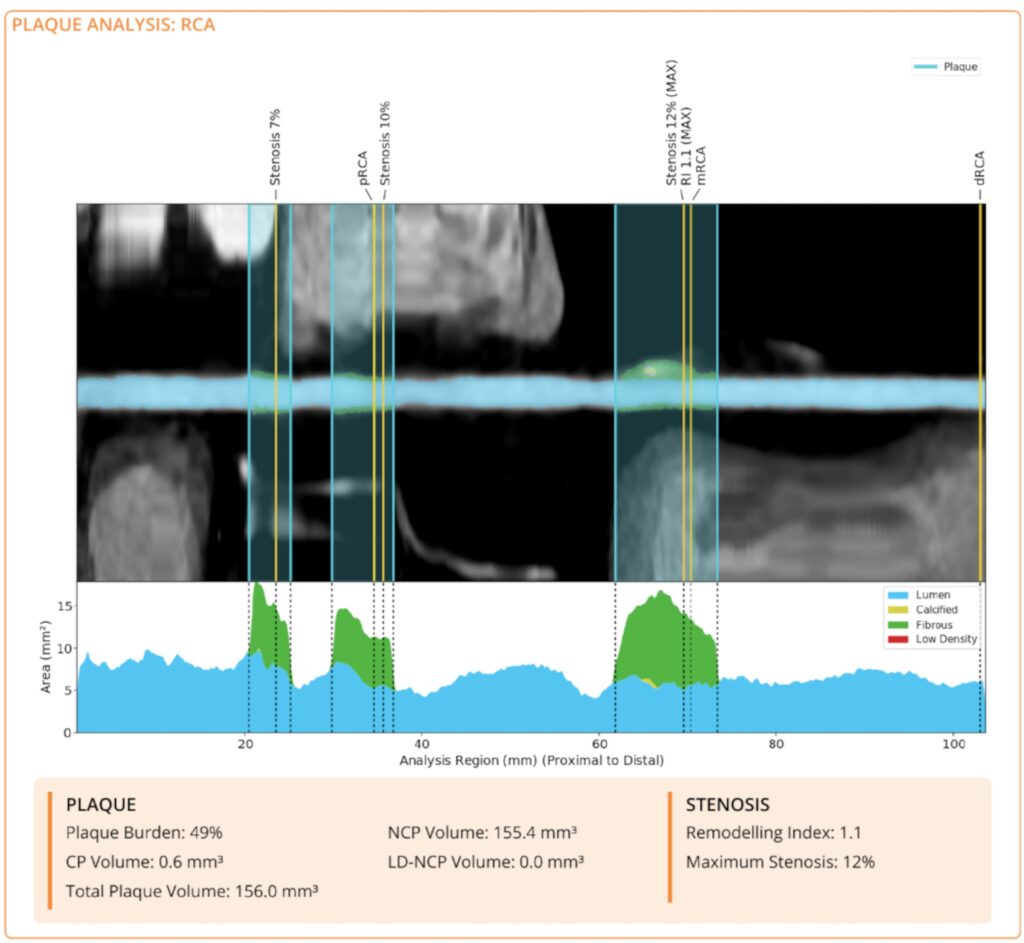
Depending on image quality and anatomy, this can provide vessel-by-vessel metrics such as:
- Total plaque volume across the coronary tree
- Non-calcified plaque volume and calcified plaque volume
- Low-density non-calcified plaque volume (a CT marker that can reflect more lipid-rich plaque biology)
- Plaque burden (the proportion of the vessel segment occupied by plaque)
- Maximum diameter stenosis (quantified maximal narrowing in a segment)
- Remodelling index (how much the vessel expands at the plaque site, a feature often seen with higher-risk plaque)
Importantly, it uses the same CTCA scan data, so there is no additional scanning.
How CaRi-Plaque fits with CaRi-Heart at CSC
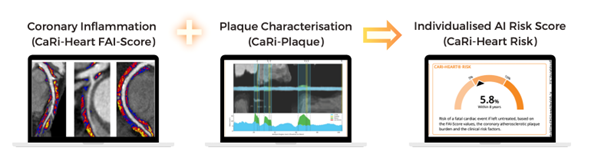
CaRi-Heart focuses on an inflammation-related signal derived from perivascular fat analysis (FAI). Plaque quantification focuses on the amount, type, and distribution of atherosclerosis. These are complementary: one reflects biological activity, the other describes the disease substrate.
At CSC, CaRi-Plaque is commonly used as an optional add-on to CaRi-Heart when deeper anatomical characterisation is likely to change management, or when standard reporting does not fully capture plaque burden and composition.
Why quantification matters clinically
Quantification is not simply “more detail”. It can add clinical value by:
1) Identifying higher-risk patients with non-obstructive disease
A patient may have only mild narrowing but still carry a meaningful plaque burden or higher-risk plaque composition. Quantification helps avoid false reassurance when the tightest stenosis is not severe.
2) Supporting more personalised prevention decisions
Objective plaque metrics can help tailor prevention intensity, including lipid targets and the threshold for combination lipid-lowering therapy, alongside structured lifestyle and blood pressure optimisation.
3) Improving reference with objective benchmarks
Where available, expressing plaque burden relative to age- and sex-adjusted reference ranges (for example, percentile rankings) can make results easier to understand and can clarify why prevention may be recommended even in the absence of severe narrowing.
4) Providing a baseline for comparison in selected cases
Repeat CTCA is not routine, but in selected patients where repeat imaging is clinically appropriate, quantitative metrics allow more meaningful comparison over time than subjective description alone.
What you receive in a CaRi-Plaque report
Your report is structured and quantitative, and may include:
- Vessel-by-vessel plaque volumes and plaque composition
- Summary measures of plaque burden
- Quantified maximal stenosis and remodelling indices (where applicable)
- A clinician-facing interpretation that integrates these findings with the CTCA context
Your cardiologist will review the findings with you and integrate them into a prevention plan.
Who is CaRi-Plaque for?
CaRi-Plaque is most useful when the clinical question is not simply “Is there a severe blockage?”, but “What is the true burden and type of coronary atherosclerosis, and how should prevention be tailored?”
It may be considered for people who:
- Have mild or non-obstructive plaque on CTCA but there is concern risk may be underestimated
- Have strong family history or multiple risk factors where intensity of prevention is uncertain
- Want a clearer baseline assessment of coronary plaque burden and phenotype to guide management decisions
Booking and enquiries
If you are interested in CaRi-Plaque, discuss it with your CSC cardiologist or contact Central Sydney Cardiology on 02 9336 2666 or email cariheart@cardiology.sydney